For Hospitals & Clinics
Your care is excellent.
Your systems are not keeping up.
Most hospitals and clinics in India are delivering good clinical care every day. But somewhere between the front desk and the discharge desk, patients are getting lost, beds are staying blocked, and the team is burning out — not because anyone is doing a bad job, but because the system around the care is not designed to grow.
That is what we fix.

Multi-specialty hospitals
Medical Directors and CMOs managing bed flow, OT utilisation, discharge discipline, and patient retention across departments.

Clinics & specialty centres
Owner-doctors running a growing practice — but spending too much time managing the business instead of treating patients.
The problem is rarely the care.
It is almost always what happens around it.
We see this in clinics and even in some of India’s best multi-specialty hospitals. The doctors are skilled. The equipment is good. Care is being delivered.
Yet a patient who is clinically ready for discharge at 10 a.m. is still in the bed at 3 p.m., because the discharge summary is pending, billing has a query, and no one owns the process.
That blocked bed delays the next admission. The next admission delays the OT schedule. The OT slips. The surgeon is frustrated. The patient waiting for surgery waits longer.
No one made a bad decision. But the system quietly lost half a day — entirely avoidable.

This is not a clinical problem. It is a system design problem.
And it is exactly what OneMedPro is built to fix.
If any of these are happening in your hospital, we can help.
Calls & Appointments
Your front desk gets 80 calls a day. 20 go unanswered. Patients who can't get through don't call back, they book somewhere else. You never see the loss because it never shows up in your data.
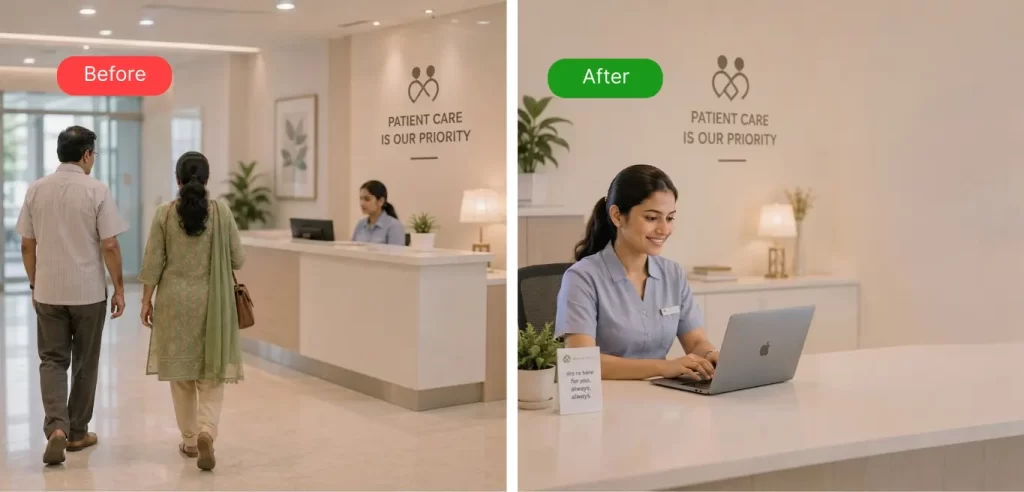
OPD Flow & Waiting
Patients wait 45 minutes past their appointment time. Staff are stressed. Doctors are running late. Complaints go to Google reviews, not to you. The reputation damage is slow but real.
Discharge & Bed Flow
Most discharges happen after 2pm. Beds sit blocked for hours after patients are clinically ready. OT schedules slip. Nobody owns the last mile between "clinically ready" and "physically gone."
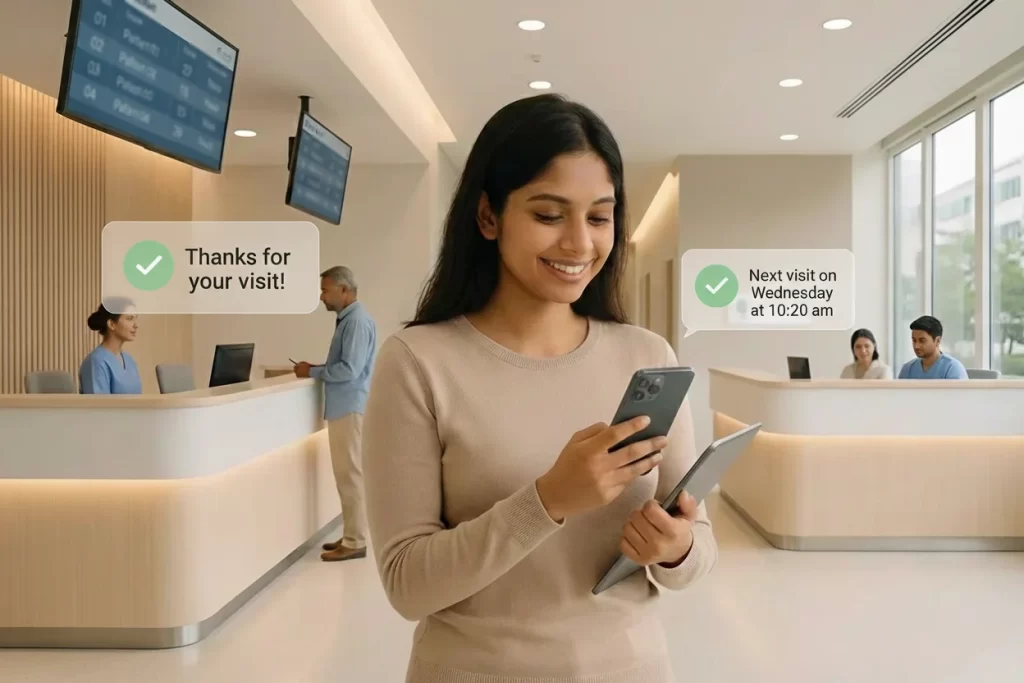
Follow-ups & Retention
Patients leave and disappear. No recall system. No follow-up calls. No way to know who came back and who didn't. Your team is too busy with today's patients to chase yesterday's.
Here is what changes, and how quickly.
We do not hand over a report and leave. We install a working system, and stay until it runs without us. Here is what that looks like in practice.
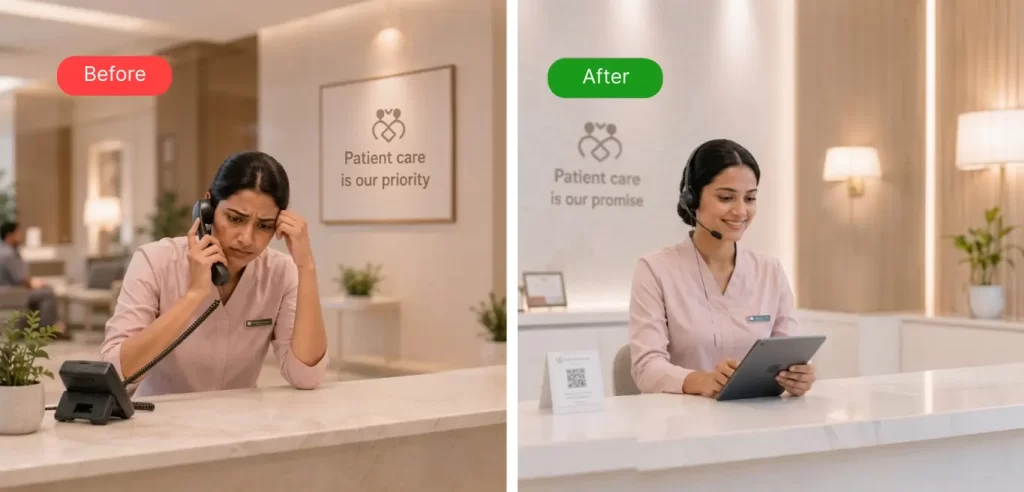
Before: Calls missed daily, no callback system
After: Every call logged, follow-up within 2 hours
A simple call-handling protocol and WhatsApp flow. Your staff owns it. It runs every day without a manager chasing it.

Before: Discharge happens whenever it happens
After: 60% of discharges complete before noon
A discharge readiness checklist, a daily 8am ward review, and clear ownership of each step. Beds free earlier. OT runs on schedule.

Before: OPD waits with no visibility
After: Average wait time tracked and managed weekly
A weekly rhythm of numbers your team reviews every Monday. Not a dashboard nobody opens, a 15-minute meeting that changes what happens that week.
Before: Patients leave and are never heard from again
After: Recall system running for 90-day and annual follow-ups
Automated WhatsApp reminders, a staff recall script, and a monthly report of who returned and who didn't. Retention becomes a number, not a hope.
Three ways to work with us.
Start with what's most urgent.
You do not have to commit to everything. Start with the one that fits your biggest gap right now, and expand from there.
ENGAGEMENT 01
OPD Growth Intensive
30 – 60 days
For clinics and hospitals where the front door is leaking — missed calls, no-shows, poor OPD flow, patients not returning. We audit, fix, install, and hand over a running system.

ENGAGEMENT 02
Clinical Growth Operating Model
60 – 90 days
For hospitals where the deeper problems are bed flow, discharge discipline, OT utilisation, and department-level accountability. A full operating model, installed, not just designed.

ENGAGEMENT 03
Grow, Scale & Stabilise
Ongoing · quarterly
For hospitals preparing to expand — new units, new locations, new service lines. We make sure the growth plan is built on a system that can scale, not one that will break under pressure.
Featured paper
“We don’t just fix hospitals. We study them.”
From Bed Occupancy to Throughput
A Consultant's Field Note
India’s hospitals already have one of the lowest average lengths of stay in the world. Yet beds remain underproductive, OTs run late, and emergency care absorbs the pressure. This paper asks why — and what to do about it.

Frequently Asked Questions
Get your questions answered here. if not write to us.
Do you work with small clinics or only big hospitals?
Yes. We support single-doctor clinics to multi-specialty hospitals. The approach is adapted to your scale and team size.
What happens in the first 2 weeks after we start?
We map your front-door flow, identify leakage points, assign ownership, install basic scripts/SOPs, and set up weekly tracking so improvements are visible immediately.
What exactly is OPD Growth Intensive?
It fixes appointment leakage—missed calls, cancellations, no-shows, weak follow-ups—and installs a weekly routine your team can run consistently.
What is CGOM and when should I choose it?
CGOM is an audit-led installation for deeper operational issues across roles and workflows. Choose it when the problem is not just OPD—it’s handoffs, SOP discipline, and accountability across the system.
How much time do you need from the doctor or leadership team?
Minimal daily time. We need one focused kickoff + a weekly 30–45 minute review to keep the rhythm strong. Execution is handled with your coordinators/front office.
Will you only advise or will you implement?
We implement. We fix what’s broken, train your team, and install a weekly cadence with tracking.
How is OneMedPro different from a hospital management consultant?
Most consultants deliver a report and leave. We install a working system, workflows, SOPs, trained staff, weekly tracking, and stay until it runs without us. The difference is in what gets left behind.
How soon will we see results?
Initial improvements typically show within 4–6 weeks (call handling, no-show recovery, follow-ups). Full stabilization varies by size, but progress is measured weekly from day one.
Is the Growth Check-up free?
Yes. It’s a short diagnostic call. Paid programs start after we agree on scope and outcomes. The check-up call is 30 minutes. No preparation needed from your side, just tell us what’s breaking and we’ll take it from there.